- Play therapy is
- A type of child counselling
- Ideal for kids 3 to 12 years old
- Allows kids to express and process their needs and experiences without needing to talk about it
- Influenced by 100 years of culminative shifts in child development research and practice
- Like talk therapy, play therapy should only be carried out by a clinician with postgraduate qualifications
- Clinicians also undertake specialist training in using play as the medium of change, and work systemically with the child’s ecosystem.
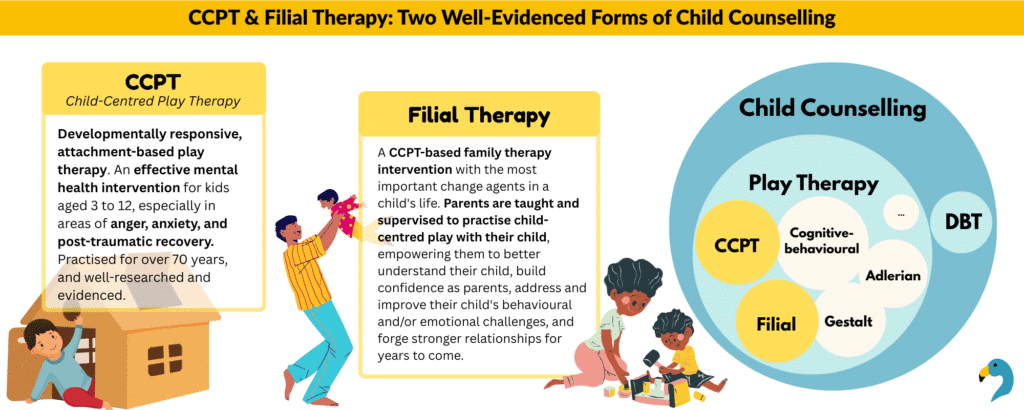
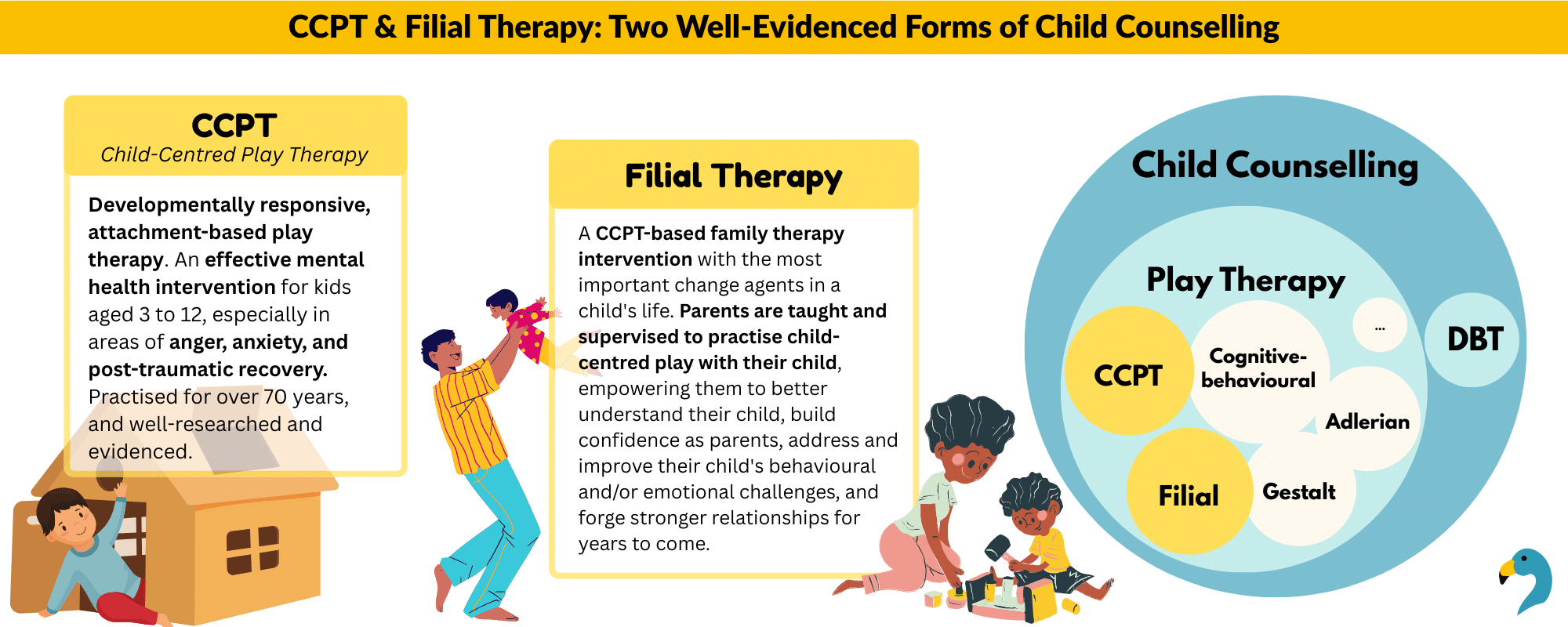
- Child-Centred Play Therapy (CCPT) and Filial Therapy are two well-researched types of play therapy
Introduction
What is play therapy? Is it “just playing”?
These are hands down the most common first questions I get from parents, teachers, and… everyone. Since the word play usually conjures up images of leisure and relaxation, it can be confusing to see it paired with therapy. If you want to find out more, you’ve come to the right place!
- If your child is struggling with their behaviour or with hard feelings, you might be considering child counselling and play therapy to support them.
- Maybe you want to find out what play therapy involves, if it’s aligned with your personal values and beliefs, and decide if play therapy is a good fit for your child.
- Or maybe you know someone who often confides in you about the challenges they face with their child, and their worries about what’s going on and what to do.
Let’s take a dive into what play therapy is – and why it’s not “just playing”.
What is Play Therapy?
Play therapy is at its core a type of child counselling. Using play therapy, children aged 3 to 12 years old can process things in the past and present using play, rather than words.
While many kinds of play therapy are available today, the most effective ones combine these core elements:
A strong therapeutic alliance, collaboration with the child’s system (parents, foster care, education, etc.), unconditional acceptance alongside safe limit-setting, a solid understanding of child development, a capacity to shift unhealthy internal thought patterns towards healthier ones, and support from current knowledge of child neurobiology.
Historical Influences in Child Counselling
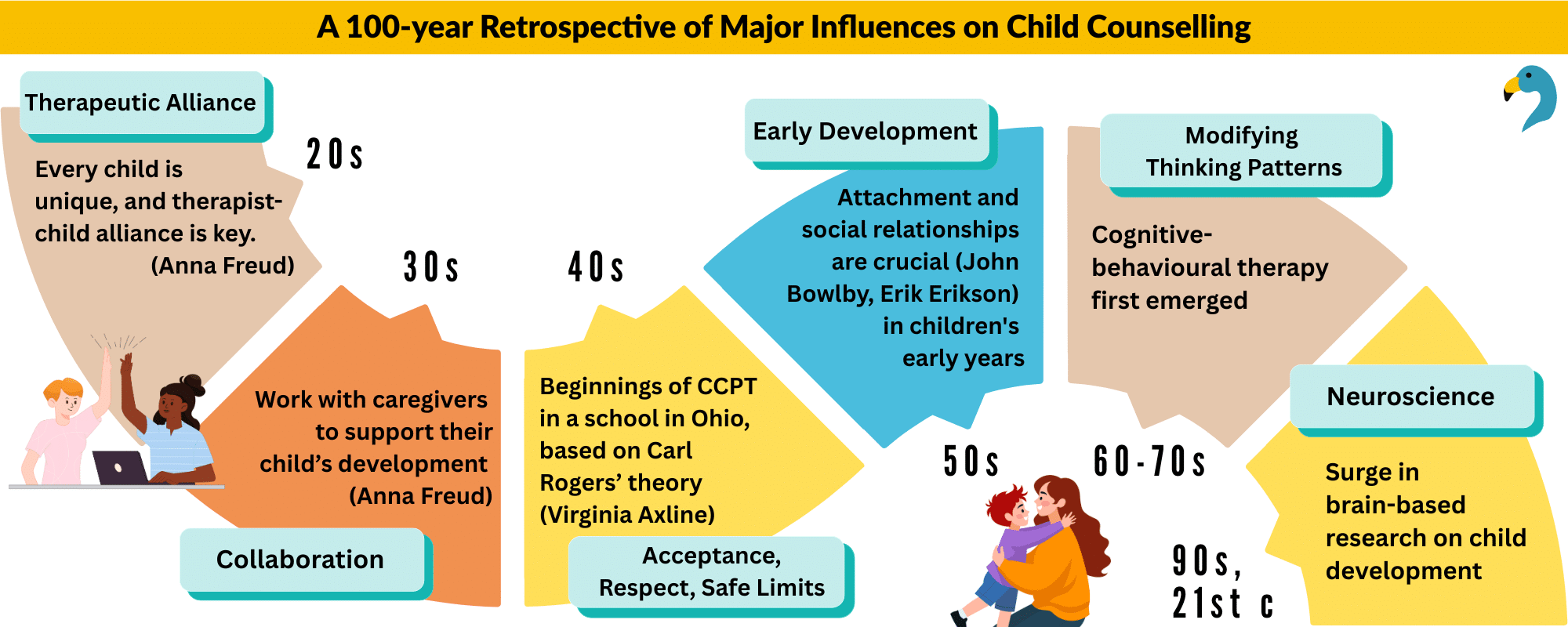
None of this came swiftly or easily. In fact, the play therapy practised today is the confluence of a whole century of major influences:
- Therapeutic Alliance: In the 1920s, Anna Freud began emphasising the therapeutic alliance, which is the warm and positive relationship between a therapist and a child. She recognised children’s need to explore and play, and tapped on this to form a therapeutic alliance, giving them the freedom to move from the couch and onto the floor, where they could more freely draw and play.
- Collaboration: In the 30s, Anna Freud was also one of the first to collaborate with a children’s caregivers, especially those with very young children. Through psychoeducation, the caregivers learnt ways to better support their child’s development, even as their children simultaneously underwent child therapy.
- Unconditional Acceptance, Respect, Safe Limits: In the 1940s, the beginnings of Child-Centred Play Therapy (CCPT) took root in Ohio. Virginia Axline, then a teacher, carried out child therapy based on Carl Rogers’ theory of unconditional positive regard – a theory which was revolutionary and hotly disputed at the time – which has today become an accepted norm in therapy.
- Early Development in Children: In the 1950s, the world began learning that attachment and social relationships are critical in children’s early years, thanks to seminal works on attachment theory (John Bowlby) and the psychosocial stages of growth (Erik Erikson). We recognise now that a child’s early emotional bonds strongly shape their future relationships. These social dynamics also influence the core beliefs that children progressively form as they grow, and thus impact how they relate to themselves and to the world.
- Modifying Thinking Patterns: From the 60s to 70s, cognitive-behavioural therapy first emerged. It involved examining thoughts, feelings, and behaviour, with a focus on changing thought patterns to reduce distress.
- Neuroscience: From the 90s and on into the 21st century, brain-based research on child development surged alongside advances in technology like functional Magnetic Resonance Imaging.
One wonderful thing about history is the satisfaction of seeing these threads come together, so we can better support children today.
Play Therapy vs Talk Therapy
Both play therapy and talk therapy should always be carried out by trained clinicians.
The effective therapist:
- Is trained clinically, with a postgraduate qualification in counselling, clinical psychology, or clinical social work
- Possesses key therapeutic capabilities which apply in both play therapy and talk therapy
Safety and trust-building is the first and most primary ingredient. With a strong therapeutic alliance and foundation established, we feel safe talking or playing through our experiences, challenges, and hopes.
Working through our experiences will at times be difficult. We are encouraged and held by the space of open-mindedness, empathy, and adaptability of the therapist, as well as helpful therapeutic interventions.
Over time, we are supported to build more helpful perspectives, connect to inner and outer resources, and begin to live in a way that makes us feel more fulfilled.
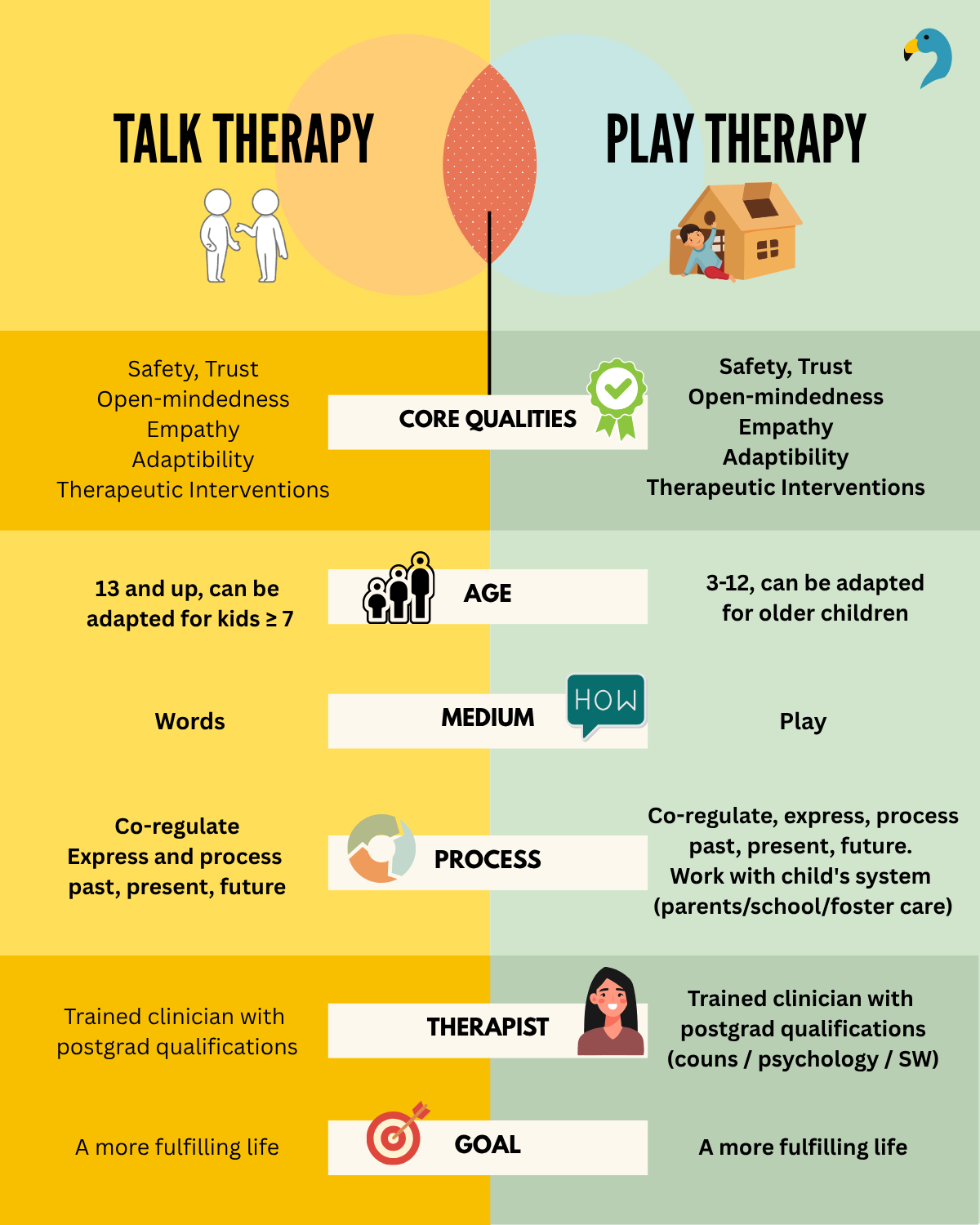
In these broad, overarching ways, the core qualities, basic therapist qualifications, and goals of talk therapy and play therapy are similar.
The key differences are in the age of clients, the medium used, the process of therapy, and the additional training required to successfully deliver play therapy:
- Age: Play therapy is used with children aged 3 to 12 years, though it can be adapted for older children to meet their specific developmental needs. Talk therapy is usually done with teenagers and adults, although some types of talk therapy have been specially adapted for use with kids as young as 6 or 7, such as dialectical behavioural therapy for children (DBT-C).
- Medium: Play is the primary medium in any play therapy, using toys and other play and expressive materials. In talk therapy, words are the primary medium.
- Process: When working with children, it is especially important to work with their ecological system, as children (as well as other vulnerable groups, e.g. severely disabled people) typically have less power and say over their lives than most adults do. There is evidence that working simultaneously with children’s parents/caregivers is one of the most crucial ingredients for long-term success in child counselling.
- Therapist qualifications: On top of postgraduate clinical training, therapists also need to complete specialist training in play therapy. This ensures they have a solid basis in the work of forming a therapeutic alliance with kids, and are trained to use play within a strong theoretical orientation to create therapeutic change.
Play therapy is not just playing.
Play is a beautiful medium to work with children to bring about therapeutic change – just make sure you choose a therapist with adequate qualifications.
Why Use Play?
At younger ages, children are still developing concrete and abstract language skills. Talking about things may (though it isn’t always) be intimidating or difficult for them. Leveraging their natural language of play helps to smoothen and ease the therapeutic process.
How many times have you summoned up all your patience, put aside your frustration, and asked a child as gently as you could:

“Why did you do that?” – Only for them to frown furiously, look down, and express general overwhelm and incapacity to talk?
It’s hard enough for us as adults to express ourselves in words when we’re upset. What more children, whose frontal lobes will only fully develop when they hit their twenties?
Play is a way for children to express their inner/outer conflicts without needing to formulate words. In fact, this already happens naturally, all the time!
Play therapy brings all this together:
- Kids naturally self-express through play, across cultures
- Kids find it fun and are intrinsically motivated to play
- Kids feel more at ease and less under pressure when working with toys and play – we enter their world, rather than making them enter our adult world
In sum, play therapy taps on play being developmentally appropriate, the main way that children naturally learn, interact with the world, and process events and feelings.
“Toys are children’s words and play is their language.”
(Garry E. Landreth, one of the most influential figures in the field of play therapy)
Play is how kids process their life experiences.
Not Just Playing: What happens in Child-Centred Play Therapy (CCPT), and How Children Progress
What Happens in Play Therapy?
There are quite a few different types of play therapy – these include Adlerian, Child-Centred, and Gestalt play therapy. What actually happens during a session depends on which type(s) of play therapy your clinician specialises in.
This article focuses on two main types of play therapy:
- Child-Centred Play Therapy (CCPT): Therapist works 1-on-1 with the child. CCPT is one of the oldest (nearly 80 years) and most well-researched and evidenced therapeutic modalities for children. It is an attachment-based play therapy, and innately responsive to children’s stage of development. It is an effective mental health intervention for kids aged 3 to 12, especially in the areas of
- anger,
- anxiety, and
- post-traumatic recovery, including significant changes in the family. It is also the primary method of child counselling in my practice.
- Filial Therapy (FT): Therapist works with both parent and child. FT is a CCPT-based family therapy intervention with the most important change agents in a child’s life – parents! Parents are taught and supervised to practise regular child-centred play with their child, empowering them to
- better understand and communicate with their child,
- build confidence as parents,
- address and improve their child’s behavioural and/or emotional challenges, and
- forge stronger relationships, supporting better success for their children and reduced parental stress for years to come.
What Happens in Child-Centred Play Therapy (CCPT)?
Child-Centred Play Therapy (CCPT) is a form of child-led play therapy.
In CCPT, playrooms are carefully curated, with a wide range of play materials that allow children to express and communicate a wide variety of feelings and challenges. This means having:
- real-life toys (e.g. toys for shopping, cooking),
- creative and expressive materials (e.g. paper, crayons, paint), and
- toys that are “scary” / support the externalisation of aggression (e.g. fierce animals, toy swords).
When children enter a CCPT playroom, the clinician (i.e. the therapist) lets them decide what toys they want to play with, and how they want to play.
The clinician pays very close attention to what the child does and feels, and skilfully and consistently supports the child’s process. We often say that the clinician is the most important toy in the playroom!
Throughout each weekly session, the clinician:
- Reflects the child’s emotions, intents, and experiences to increase the child’s self-insight to the child,
- Scaffolds them to make their own decisions,
- Demonstrates acceptance of challenging emotions, and
- Safely sets boundaries in the face of unsafe behaviour. When needed, the clinician sets limits calmly but firmly, with no anger, and with clear consequences (e.g. the toy/material might become out of bounds for the rest of the session, or in extenuating cases, the play session might end early).
How Children Progress Through CCPT
In CCPT, children often progress, usually chronologically, through 4 stages:
- The Warm-up Stage
- The “Aggressive” Stage
- The “Regressive” Stage
- The Mastery Stage
Let’s go through each of these briefly.
- The Warm-up Stage
When children first enter a CCPT playroom, they begin a warm-up stage. It takes time before the constancy of empathy, attention, and understanding can sink in and be accepted.
How long this takes differs from child to child. Some kids immediately feel comfortable enough to play freely in their first couple of sessions. Others take a longer time – up to 10 sessions – to feel safe enough to show who they are in their play. This is particularly true for children with big attachment wounds.
Given that we live in a world where children are supervised and guided (often with the best intentions) more than ever, it is understandable that children may initially find it hard to believe that they can truly self-express and make their own choices without being corrected, punished, or losing their relationship with an adult.
- The “Aggressive” Stage
As a child gets more comfortable with the therapist and in the playroom, they transition into the aggressive stage. During this stage, children may act out inner or outer experiences of aggression through fantasy play scenarios, or through the way they challenge, compete, or play games with the therapist.
This is where a child with oppositional tendencies, defiance, and challenges with anger would spend a longer time working through, with the therapist’s support.
- The “Regressive” Stage
The regressive stage goes even deeper; the child now has enough of a sense of control to work on issues that are tied to their most vulnerable needs. With a deep sense of trust in the therapist, the child can now express, tolerate, and accept difficult feelings around themes such as dependency, separation, grief, protection, and self-worth.
Children with trauma backgrounds may spend a longer time in this stage, processing attachment wounds.
As children grow more comfortable with expressing their needs, they may also bring this into daily life outside the playroom and display regressive behaviour in real life. Parents can be reassured that this is natural, and is a passing phase.
- The Mastery Stage
Having done an incredible amount of work, the child finally integrates these positive changes during the mastery stage. Children now display a stronger self-confidence and a more positive regard for others; they value relationships more and this shows up in the way they play in the playroom.
Outside the playroom, this is backed up by parallel changes, as the child achieves most or all of the therapeutic goals that were set out at the beginning. This often happens slightly after changes are seen in the playroom.
To ensure these changes are truly integrated, they continue to spend some time in play therapy during this Mastery stage. The idea of ending is then introduced, and children are told exactly how many sessions they have left, giving them the time they need to process the ending of the play therapy relationship.
Does Play Therapy Really Work?
How does Child-Centred Play Therapy Change Children?
In the child-centred play setting, children feel fully accepted. They build up a strong sense of internal safety, and learn that they are okay as they are.
With the clinician’s consistent presence, children who go through CCPT:
- Gain insight into, and learn to self-regulate and co-regulate as they tolerate and accept their own emotions.
- Nurture self-directedness and build up a bigger capacity to attempt challenging things. As a result, they become more resilient, and their confidence improves.
- Learn to take responsibility for their own actions.
- Internalise that others can be firm and keep them safe, without escalating emotions and using fear/anger tactics (parents/teachers/caregivers – we all know how hard this can be when we’re trying to juggle a million other things!).
It’s not only the child who learns. It’s also you, the parent/caregiver, the most important person in your child’s life.
- The clinician is trained to understand the meaning of a child’s play as well as
- During regular parent consultations, the clinician discusses these underlying patterns and works with the parent/caregiver to come up with possible strategies to further support the child.
Who Can Play Therapy Help?
Play therapy, and CCPT in particular, is a proven method that is well-researched. If your child struggles with angry outbursts at home or in school, or has high anxiety that is limiting their enjoyment of life, or is recovering from a traumatic experience, know that there is hope for them!
Play therapy has been found effective at reducing symptoms in kids with anger, anxiety, and post-traumatic challenges.
It may seem somewhat strange to our adult brains that play therapy works at all, but on top of play being a developmentally appropriate medium for child therapy, play therapy also fulfils two key characteristics for optimal child development that are backed by science:
- Play therapy fundamentally involves forming a secure attachment; and
- Playing stimulates both sides of the brain.
Based on the latest neurobiological research, the freedom to play and the presence of secure attachment(s) are EXACTLY what best helps kids grow physically, cognitively, and emotionally.
Final Thoughts
Play therapy is a structured therapeutic process – a way to help children using their own natural language of play.
Neurobiological research and brain imagining studies now back up the CCPT practices that have been clinically effective and helped kids get better since the 1940s.
The conditions of secure attachment, child-led activities and the medium of play so often work – because under these conditions our children’s brains become more amenable to healing, learning, and growth. Like flowers, they can blossom from the inside out.
References
- Koocher, G. P., & D’Angelo, E. (1992). Evolution of practice in child psychotherapy.
- Grimwade, J. (2023). Lessons from the Twentieth Century for Child and Adolescent Mental Health Practice in the Twenty-First Century.
- Craighead, W. E. (2019). A brief clinical history of cognitive-behavior therapy with children.
- McLeod, S. (2025). John Bowlby’s attachment theory.
- Orenstein, G. A., & Lewis, L. (2022). Erikson’s stages of psychosocial development.
- Witkin, M. (2025). Anna Freud (1895-1982): Child psychoanalysis and child psychology.